Leonard Coleman’s great-grandfather, Dr. John Thomas Bolton, was born in Georgia, March 22, 1839, the son of Colonel Charles and Mary Bolton. In 1846 he moved with his family to a large plantation near Wharton, Texas.
After graduating from a medical and surgical school of New Orleans, Dr. Bolton enlisted as a private in Company C of the Thirty-fifth Texas Calvary. His medical education had been inadequate and brief. He received very little clinical experience, and was given no laboratory instruction. The medical school in New Orleans had no microscope, laryngoscope, stethoscope, or ophthalmoscope. No physician—all know as surgeons then—used hypodermic syringes to administer medicine.
Dr. Bolton’s first experience as a wartime surgeon remained etched in his memory as lifelong recurrent nightmares. Summoned at a gallop to a field hospital, he passed wounded soldiers lying where they had fallen several days earlier. Too wounded to crawl, they writhed in agony and with parched lips cried for water. Some of the less severely injured had managed to pull themselves under the shade of trees or to a small creek where they soaked in muddy water. The rotting corpses of their dead comrades surrounded them. No assistance was in sight.
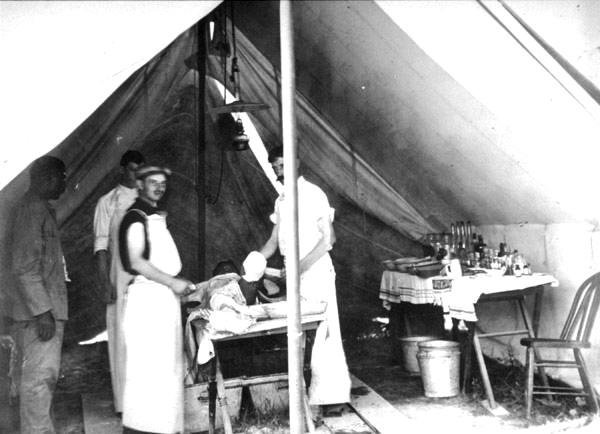
Riding on as he had been commanded, Dr. Bolton found conditions little better at the field hospital. Filth was all around. Flies circled the severed limbs that had been thrown helter-skelter in a pile next to the surgical tent. Just in front of the open-flapped tent, a patient had been placed on the operating table consisting of wooden planks positioned across two barrels. A blood-saturated oilcloth covered the table. A bucket on the ground below caught free-flowing blood during the amputations. Congealed blood matted everything.
Approaching the surgical tent, Dr. Bolton became alarmed by his mounting anxiety. He had no idea how to do an amputation. He had never seen one. He suppressed his own vomit with the first glimpse of the brigade surgeon who, having just completed an operation, stood holding a bloody knife. His bare arms and linen apron were smeared with blood.
Pride in his heritage enabled Dr. Bolton to dismount. Arriving at the operating table the stench nearly overpowered him, and for a few brief seconds he felt he was going to faint when he heard the words that he later recounted to his grandchildren, “Your pallor tells me you have no experience in this kind of thing. So I’ll show you how to do one. Then you can do one. And when a young doctor rides over the horizon you can show him how to do one.”
“See one, do one, teach one,” Dr. Bolton would say. “That’s the best way for anyone to learn—whether doing surgery, managing a bank or raising cotton.”
Immediately the experienced surgeon began to demonstrate the art of wartime medicine to the boyish-appearing Dr. Bolton. While one assistant applied a Petit-type screw tourniquet on the soldier’s thigh, another steadied the leg. A third administered chloroform.
Despite romanticized tales of soldiers biting a bullet or getting rip-roaring drunk prior to undergoing the knife, surgical anesthesia was universally applied during most of the war. The Union physician, Dr. Samuel Gross in his Manual of Military Surgery had advocated avoiding chloroform because he felt anesthesia produced shock. In his surgical manual, Dr. John Julian Chisholm of the Medical College of South Carolina disagreed: “Whenever operations are to be performed chloroform should be administered. It is a remedy which the surgeon should never be without.” Not long after the beginning of the conflict, surgeons from both from the North and South were using chloroform, a wounded soldier’s best friend.
Although ether, a longer acting anesthesia, was also available, chloroform became the anesthesia of choice because of its non-flammability properties and speed of action. The sweetish-smelling liquid could be sprinkled on a handkerchief that was placed over the soldier’s nose and mouth.
Most Confederate surgeons preferred the use of a small funnel. Chloroform was dripped through the funnel’s neck onto a sponge within the wide portion of the device. The bottom of the funnel was placed over the patient’s face. Air, which entered through the funnel neck, mixed with the chloroform, provided an unsophisticated means of anesthesia. As soon as the patient became limp, the amputation quickly proceeded.
As the surgeon began to cut, he instructed Dr. Bolton, “I’ve read that the Union physicians prefer the flap operation. They make crescent shaped cuts, side to side. This technique provides more soft tissue and skin coverage, making a better stump. But in the opinion of Dr. Chisholm, the larger wound that this method requires leads to more bleeding and infection. We Confederates favor the circular technique. The skin is incised and folded back, like this. Now you cut the muscle and then take the saw to the bone. Finally bring the cuff of skin down over the stump and close the wound with these sutures.”
So fast were the experienced surgeon’s hands that by the time the quick acting chloroform had worn off, the operation had been completed. “Now,” the surgeon said, “It’s your turn to do one.”
Many years later, Dr. Bolton admitted that he wanted to beg the surgeon to perform the operation for him, but the expectation in the doctor’s voice and the penetration of his eyes indicated that groveling would do no good. With trembling hands, Dr. Bolton removed the limb.
Soon another table was constructed, three additional assistants were recruited and the two surgeons worked side-by-side into the night. Taking very few breaks, they completed their work by the second evening. By that time the mounting pile of amputated limbs had reached five feet. Exhausted, Dr. Bolton staggered to a yaupon thicket and vomited.
Dr. Bolton became so repelled with amputating the limbs of fallen comrades and worse—the maniacal ravings, bitter sobs, and piteous cries of those recovering and dying in the field hospitals—that, after the war, he turned his scalpel in for a plowshare and never practiced medicine again.
Purulent wounds, pyemia (blood poisoning), gangrene, and osteomyelitis were behind him. Prosperity and civil service lay ahead. He became a city icon in the early years of Wharton‘s history. In addition to managing his plantation, he was elected county treasurer, county commissioner, and city alderman.